Predictores clínicos de revascularización quirúrgica en pacientes cursando internación por síndromes coronarios agudos sin elevación del segmento ST - Registros Buenos Aires I y ReSCAR22
DOI:
https://doi.org/10.47487/apcyccv.v5i1.333Palabras clave:
Revascularización Miocárdica, Enfermedad Coronaria, Síndrome Coronario Agudo, ArgentinaResumen
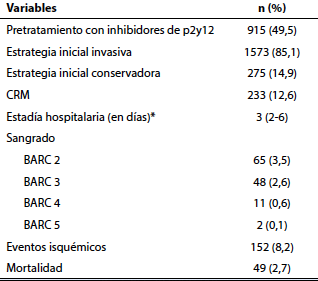
Objetivo. Identificar predictores independientes de cirugía de revascularización miocárdica (CRM) en pacientes con síndrome coronario agudo sin elevación del segmento ST (SCASEST) del mundo real. Materiales y métodos. Se realizó un análisis preespecificado de forma individual de pacientes con SCASEST, a partir de dos registros argentinos prospectivos entre 2017 y 2022. Se analizó la diferencia en las características basales entre los pacientes que requirieron CRM y los que no requirieron esta intervención. Luego, se realizó un análisis de regresión logística para determinar predictores independientes en los pacientes que recibieron CRM como método de revascularización. Resultados. Se incluyeron 1848 pacientes con una mediana de edad de 54,8 (rango intercuartílico [RIC]): 53,7-56) años y una fracción de eyección de 42,1% (RIC: 41,2-43,1). Un total de 233 pacientes requirieron CRM (12,6%). Las características basales entre ambos grupos fueron similares, excepto en los pacientes que requirieron CRM, que mostraron ser más jóvenes (51,5 vs. 55,7 años; p=0,010), más frecuentemente diabéticos (38,2% vs. 25,7%; p=0,001) y hombres (90,1% vs. 73,7%; p=0,001); además, presentaron en menor medida, una cirugía cardíaca previa (2,1% vs. 11,2%; p=0,011). Luego del análisis multivariable, se asociaron de forma independiente con la CRM: la edad (Odds Ratio [OR]: 0,99, intervalo de confianza [IC] al 95%: 0,98-0,99; p=0,008), sexo masculino (OR: 3,08, IC 95%: 1,87-5,1; p=0,001), antecedente de CRM previa (OR: 0,14, IC 95%: 0,05-0,30; p=0,001) y diabetes (OR: 1,84, IC 95%: 1,31- 2,57; p=0,001). Conclusiones. En este análisis de dos registros de SCASEST, la edad más joven, el sexo masculino, el diagnóstico de diabetes y la ausencia de cirugía previa, fueron predictores independientes del requerimiento de CRM durante la internación.
Descargas
Referencias
Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention. 2019;14(14):1435-1534. doi: 10.4244/EIJY19M01_01.
Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e4-e17. doi: 10.1161/CIR.0000000000001039.
Gaudino M, Hameed I, Farkouh ME, Rahouma M, Naik A, Robinson NB, et al. Overall and Cause-Specific Mortality in Randomized Clinical Trials Comparing Percutaneous Interventions With Coronary Bypass Surgery: A Meta-analysis. JAMA Intern Med. 2020;180(12):1638-1646. doi: 10.1001/jamainternmed.2020.4748.
Palm DS, Drame A, Moliterno DJ, Aguilar D. Acute Coronary Syndromes Among Patients with Prior Coronary Artery Bypass Surgery. Curr Cardiol Rep. 2022;24(11):1755-1763. doi: 10.1007/ s11886-022-01784-4.
Ram E, Sternik L, Moshkovitz Y, Iakobishvili Z, Zuroff E, Peled Y, et al. Coronary Artery Bypass Grafting Following Acute Coronary Syndrome: Impact of Gender. Semin Thorac Cardiovasc Surg. 2022;34(3):920–9. doi: 10.1053/j.semtcvs.2021.07.015.
Godoy LC, Lawler PR, Farkouh ME, Hersen B, Nicolau JC, Rao V. Urgent Revascularization Strategies in Patients With Diabetes Mellitus and Acute Coronary Syndrome. Can J Cardiol. 2019;35(8):993-1001. doi: 10.1016/j.cjca.2019.03.010.
Hadaya J, Sanaiha Y, Tran Z, Downey P, Shemin RJ, Benharash P. Timing of Coronary Artery Bypass Grafting in Acute Coronary Syndrome: A National Analysis. Ann Thorac Surg. 2022;113(5):1482- 1490. doi: 10.1016/j.athoracsur.2021.05.057.
Hwang B, Williams ML, Tian DH, Yan TD, Misfeld M. Coronary artery bypass surgery for acute coronary syndrome: A network meta- analysis of on-pump cardioplegic arrest, off-pump, and on-pump beating heart strategies. J Card Surg. 2022;37(12):5290-5299. doi: 10.1111/jocs.17149.
Costabel JP, Zaidel E, Rivero M, Gomez I, Perez G. Registro multicéntrico prospectivo de pacientes hospitalizados por síndrome coronario agudo sin elevación del segmento ST en centros de alta complejidad. Resultados intrahospitalarios y evolución a 6 meses (Buenos Aires I). Rev argent cardiol. 2020;88(4):308-16. doi: 10.7775/ rac.es.v88.i4.18501.
Rivero M, Feder J, Procopio G, Gingins M, Souto JM, Villarreal R, et al. Registro de síndromes coronarios agudos en centros de alta complejidad de Argentina. ReSCAR 2022. Rev Argent Cardiol. 2023;91:205-11. doi: 10.7775/rac.es.v91.i3.20631.
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. 2018;138(20):e618-e651. doi: 10.1161/ CIR.0000000000000617.
Fox KA, Eagle KA, Gore JM, Steg PG, Anderson FA; GRACE and GRACE2 Investigators. The Global Registry of Acute Coronary Events, 1999 to 2009--GRACE. Heart. 2010;96(14):1095-101. doi: 10.1136/hrt.2009.190827.
Carvalho JF, Belo A, Congo K, Neves D, Santos AR, Piçarra B, et al. Left main and/or three-vessel disease in patients with non-ST- segment elevation myocardial infarction and low-risk GRACE score: Prevalence, clinical outcomes and predictors. Rev Port Cardiol (Engl Ed). 2018;37(11):911-919. doi: 10.1016/j.repc.2018.03.016.
Fox KA, Steg PG, Eagle KA, Goodman SG, Anderson FA Jr, Granger CB, et al. Decline in rates of death and heart failure in acute coronary syndromes, 1999-2006. JAMA. 2007;297(17):1892-900. doi: 10.1001/jama.297.17.1892.
SmilowitzNR,MahajanAM,RoeMT,HellkampAS,ChiswellK,GulatiM, et al. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With the Guidelines). Circ Cardiovasc Qual Outcomes. 2017;10(12):e003443. doi: 10.1161/CIRCOUTCOMES.116.003443.
Porter A, Paradkar A, Goldenberg I, Shlomo N, Cohen T, Kornowski R, et al. Temporal Trends Analysis of the Characteristics, Management, and Outcomes of Women With Acute Coronary Syndrome (ACS): ACS Israeli Survey Registry 2000-2016. J Am Heart Assoc. 2020;9(1):e014721. doi: 10.1161/JAHA.119.014721.
Farooq V, Van Klaveren D, Steyerberg EW, Meliga E, Vergouwe Y, Chieffo A, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: Development and validation of SYNTAX score II. The Lancet. 2013;381(9867):639-50. doi: 10.1016/S0140-6736(13)60108-7.
Wang R, Tomaniak M, Takahashi K, Gao C, Kawashima H, Hara H, et al. Impact of chronic obstructive pulmonary disease on 10-year mortality after percutaneous coronary intervention and bypass surgery for complex coronary artery disease: insights from the SYNTAX Extended Survival study. Clin Res Cardiol. 2021;110(7):1083- 1095. doi: 10.1007/s00392-021-01833-y.
Ono M, Serruys PW, Hara H, Kawashima H, Gao C, Wang R, et al. 10-Year Follow-Up After Revascularization in Elderly Patients With Complex Coronary Artery Disease. J Am Coll Cardiol. 2021;77(22):2761-2773. doi: 10.1016/j.jacc.2021.04.016.
Tesauro M, Mauriello A, Rovella V, Annicchiarico-Petruzzelli M, Cardillo C, Melino G, et al. Arterial ageing: from endothelial dysfunction to vascular calcification. J Intern Med. 2017;281(5):471- 482. doi: 10.1111/joim.12605.
Farkouh ME, Domanski M, Dangas GD, Godoy LC, Mack MJ, Siami FS, et al. Long-Term Survival Following Multivessel Revascularization in Patients With Diabetes: The FREEDOM Follow-On Study. J Am Coll Cardiol. 2019;73(6):629-638. doi: 10.1016/j.jacc.2018.11.001.
Kapur A, Hall RJ, Malik IS, Qureshi AC, Butts J, de Belder M, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol. 2010;55(5):432-40. doi: 10.1016/j. jacc.2009.10.014.
Mamet H, Petrie MC, Rocchiccioli P. Type 1 diabetes mellitus and coronary revascularization. Cardiovasc Endocrinol Metab. 2019;8(1):35-38. doi: 10.1097/XCE.0000000000000166.
FarkouhME,DomanskiM,SleeperLA,SiamiFS,DangasG,MackM, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012 Dec;367(25):2375-84. doi: 10.1056/ NEJMoa1211585.
Gholap NN, Achana FA, Davies MJ, Ray KK, Gray L, Khunti K. Long- term mortality after acute myocardial infarction among individuals with and without diabetes: A systematic review and meta-analysis of studies in the post-reperfusion era. Diabetes Obes Metab. 2017;19(3):364-374. doi: 10.1111/dom.12827.
HeadSJ,DavierwalaPM,SerruysPW,RedwoodSR,ColomboA,Mack MJ, et al. Coronary artery bypass grafting vs. percutaneous coronary intervention for patients with three-vessel disease: final five-year follow-up of the SYNTAX trial. Eur Heart J. 2014;35(40):2821-30. doi: 10.1093/eurheartj/ehu213.
Descargas
Publicado
Número
Sección
Licencia
Derechos de autor 2024 La revista es titular de la primera publicación, luego el autor dando crédito a la primera publicación.

Esta obra está bajo una licencia internacional Creative Commons Atribución 4.0.