When beta-blocker unmasks the diagnosis: pheochromocytoma mimicking acute coronary syndrome. A case report
DOI:
https://doi.org/10.47487/apcyccv.v7i1.574Keywords:
Pheochromocytoma, Acute Coronary Syndrome, Adrenergic Beta-AntagonistsAbstract
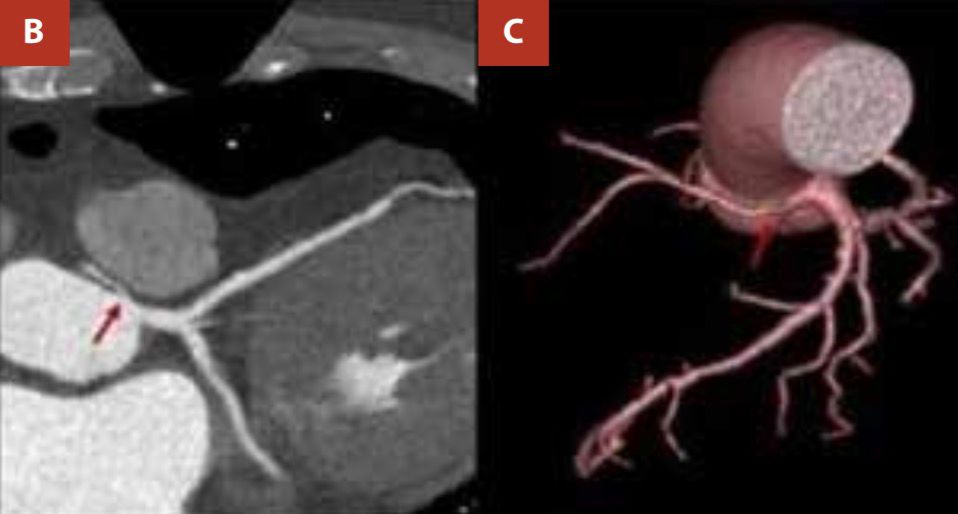
Pheochromocytoma is a catecholamine-producing neuroendocrine neoplasm classically associated with secondary hypertension. We describe the case of a 63-year-old male who presented with intermittent precordial discomfort, paroxysmal hypertensive episodes, and a mild rise in cardiac troponin levels. He was referred to our institution with a presumptive diagnosis of acute coronary syndrome. Serial admission electrocardiograms showed no dynamic ischemic changes, and transthoracic echocardiography demonstrated preserved global systolic function without regional wall motion abnormalities. A noninvasive ischemic workup was therefore planned. Before performing coronary computed tomographic angiography (CCTA), the patient received propranolol, after which he developed a hypertensive crisis accompanied by recurrent precordial pain; an identical episode occurred following a second beta-blocker dose. CCTA ruled out flow-limiting coronary artery stenoses. In view of the clinical context, pheochromocytoma was suspected. Contrast-enhanced abdominal computed tomography identified a left adrenal mass, and urinary metanephrines were elevated. The patient underwent adrenalectomy, and histopathological examination confirmed a benign pheochromocytoma. Postoperative recovery was uneventful, and the patient remains asymptomatic at follow-up.
Downloads
References
Safwat AS, Bissada NK, Seyam RM, Sobhi SA, Hanash KA. The clinical spectrum of phaeochromocytoma: analysis of 115 patients. BJU Int. 2008;101(12):1561-4. doi: 10.1111/j.1464-410X.2008.07430.x.
Y-Hassan S, Falhammar H. Cardiovascular manifestations and complications of pheochromocytomas and paragangliomas. J Clin Med. 2020;9(8):2435. doi: 10.3390/jcm9082435.3.
Strong VE, Kennedy T, Al-Ahmadie H, Tang L, Coleman J, Fong Y, et al. Prognostic indicators of malignancy in adrenal pheochromocytomas: clinical, histopathologic, and cell cycle/apoptosis gene expression analysis. Surgery. 2008 Jun;143(6):759-68. doi: 10.1016/j. surg.2008.02.007.
Wu HY, Cao YW, Gao TJ, Fu JL, Liang L. Pheochromocytoma in a 49-year-old woman presenting with acute myocardial infarction: a case report. World J Clin Cases. 2021;9(15):3752-7. doi: 10.12998/ wjcc.v9.i15.3752.
Baguet JP, Hammer L, Mazzuco TL, Chabre O, Mallion JM, Sturm N, et al. Circumstances of discovery of phaeochromocytoma: a retrospective study of 41 consecutive patients. Eur J Endocrinol. 2004;150(5):681-6. doi: 10.1530/eje.0.1500681.
Tagle V Rodrigo, Acosta V Pamela, Valdés S Gloria. Orthostatic hypotension as an unusual manifestation of pheochromocytoma: Report of one case. Rev. méd. Chile. 2003;131(12):1429-1433.
Liao WB, Liu CF, Chiang CW, Kung CT, Lee CW. Cardiovascular manifestations of pheochromocytoma. Am J Emerg Med. 2000;18(6):622-5. doi: 10.1053/ajem.2000.7341.
Gu YW, Poste J, Kunal M, Schwarcz M, Weiss I. Cardiovascular manifestations of pheochromocytoma. Cardiol Rev. 2017;25(5):215- 22. doi: 10.1097/CRD.0000000000000141.
Prejbisz A, Lenders JW, Eisenhofer G, Januszewicz A. Cardiovascular manifestations of phaeochromoc ytoma. J H yper tens. 2011;29(11):2049-60. doi: 10.1097/HJH.0b013e32834a4ce9.
Faridi SH, Harris SH, Afrose R, Siddiqui B, Ashraf H. Bilateral pheochromocytoma: an atypical cause of myocardial infarction in a young male. World J Endoc Surg. 2021;13(2):64-7. doi: 10.5005/jp-journals-10002-1408.
Szatko A, Glinicki P, Gietka-Czernel M. Pheochromocytoma/ paraganglioma-associated cardiomyopathy. Front Endocrinol (Lausanne). 2023;14:1204851. doi: 10.3389/fendo.2023.1204851.
Demir M, Özbek M, Güzel T, Aktan A. Unusual case report of malignant pheochromocytoma presenting with STEMI. Eur Heart J Case Rep. 2023;7(7):ytad249. doi: 10.1093/ehjcr/ytad249.
Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. ESC Scientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-826. doi: 10.1093/eurheartj/ehad191.
Gaudino M, Di Franco A, Arbustini E, Bacha E, Bates ER, Cameron DE, et al. Management of adults with anomalous aortic origin of the coronary arteries: state-of-the-art review. J Am Coll Cardiol. 2023;82(21):2034-53. doi: 10.1016/j.jacc.2023.08.012.
Bessell-Browne R, O’Malley ME. CT of pheochromocytoma and paraganglioma: risk of adverse events with i.v. administration of nonionic contrast material. AJR Am J Roentgenol. 2007;188(4):970-4. doi: 10.2214/AJR.06.0827.
Chrisoulidou A, Kaltsas G, Ilias I, Grossman AB. The diagnosis and management of malignant phaeochromocytoma and paraganglioma. Endocr Relat Cancer. 2007;14(3):569-85. doi: 10.1677/ERC-07-0074.
Cano Megías M, Rodríguez Puyol D, Fernández Rodríguez L, Sención Martínez GL, Martínez M. Feocromocitoma-paraganglioma: del diagnóstico bioquímico al genético. Nefrologia. 2016;36(5):481-8. doi: 10.1016/j.nefro.2016.03.010.
Worrest TC, Gilbert EW, Sheppard BC. Pheochromocytoma: 20 years of improving surgical care. Am J Surg. 2019;217(5):967-9. doi: 10.1016/j. amjsurg.2019.03.016.
Fang F, Ding L, He Q, Liu M. Preoperative management of pheochromocytoma and paraganglioma. Front Endocrinol (Lausanne). 2020;11:586795. doi: 10.3389/fendo.2020.586795.
Petrák O, Krátká Z, Holaj R, Zítek M, Nguyen Nikrýnová T, Klímová J, et al. Cardiovascular complications in pheochromocytoma and paraganglioma: does phenotype matter? Hypertension. 2024;81(3):595-603. doi: 10.1161/HYPERTENSIONAHA.123.21902.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 The journal is headline of the first publication, then the author giving credit to the first publication.

This work is licensed under a Creative Commons Attribution 4.0 International License.