Mixed shock: from pathophysiology to clinical practice
DOI:
https://doi.org/10.47487/apcyccv.v7i1.567Keywords:
Shock, Vasodilation, Heart FailureAbstract
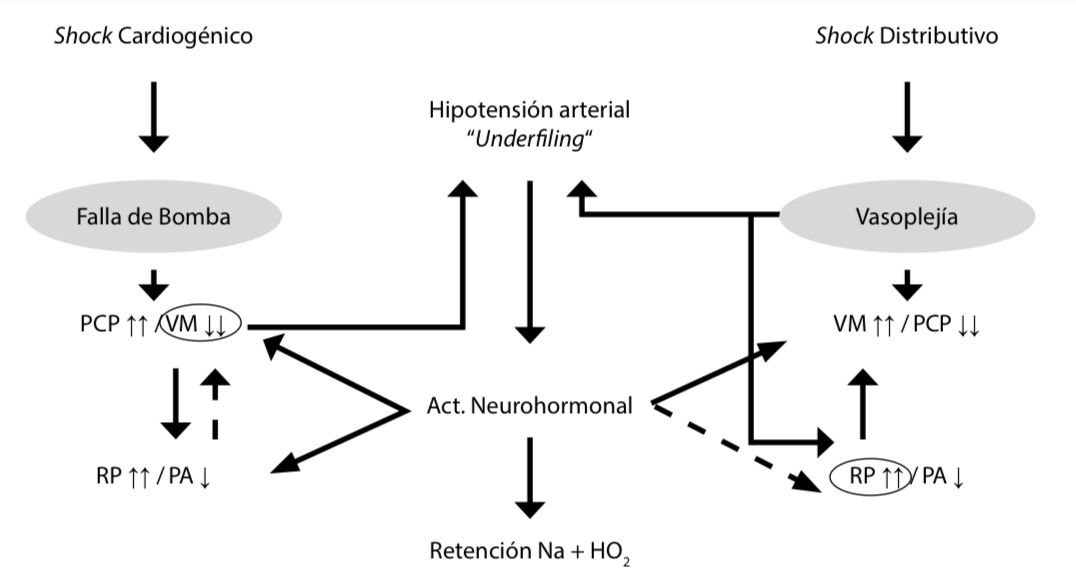
Mixed shock represents a complex haemodynamic entity arising from a variable combination of impaired contractility and vasoplegia. Its clinical recognition is challenging, as it may appear as an intermediate state in the evolution of cardiogenic or distributive shock, or result from the simultaneous coexistence of distinct pathophysiological mechanisms. Neurohormonal activation, which is common across both ends of the shock spectrum, contributes to fluid retention and further deterioration of circulatory function. Although pathophysiological interpretation is essential to guide management, it may be constrained by the temporal overlap of haemodynamic events. In clinical practice, the optimal approach integrates goal-directed haemodynamic correction with continuous bedside assessment of tissue perfusion. Pharmacological selection should account for the interaction between myocardial contractility and vascular tone, prioritising agents with combined or complementary effects. In this context, clinical judgement grounded in a sound understanding of pathophysiology remains the decisive tool in the management of mixed shock.
Downloads
References
Berg DD, Bohula EA, Patel SM, Alfonso CE, Alviar CL, Baird-Zars VM, et al. Epidemiology of cardiogenic shock using the Shock Academic Research Consortium (SHARC) consensus definitions. Eur Heart J Acute Cardiovasc Care. 2024;13(10):709-14. doi: 10.1093/ehjacc/ zuae098.
Jentzer JC, Berg DD, Chonde MD, Dahiya G, Elliott A, Rampersad P, et al. Mixed Cardiogenic-Vasodilatory Shock: Current Insights and Future Directions. JACC Adv. 2025;4(1):101432. doi: 10.1016/j. jacadv.2024.101432.
Baldetti L, Gallone G, Filiberti G, Pescarmona L, Cesari A, Rizza V, et al. Mixed Shock Complicating Cardiogenic Shock: Frequency, Predictors, and Clinical Outcomes. Circ Heart Fail. 2024;17(7):e011404. doi: 10.1161/CIRCHEARTFAILURE.123.011404.
Kunkel JB, Josiassen J, Helgestad OKL, Schmidt H, Holmvang L, Jensen LO, et al. Inflammatory response by 48 h after admission and mortality in patients with acute myocardial infarction complicated by cardiogenic shock. Eur Heart J Acute Cardiovasc Care. 2023;12(5):306- 14. doi: 10.1093/ehjacc/zuad018.
Kohsaka S, Menon V, Lowe AM, Lange M, Dzavik V, Sleeper LA, et al. Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock. Arch Intern Med. 2005;165(14):1643-50. doi: 10.1001/archinte.165.14.1643.
Meyer NJ, Prescott HC. Sepsis and Septic Shock. N Engl J Med. 2024;391(22):2133-46. doi: 10.1056/NEJMra2403213.
Jentzer JC, Szekely Y, Burstein B, Ballal Y, Kim EY, van Diepen S, et al. Peripheral blood neutrophil-to-lymphocyte ratio is associated with mortality across the spectrum of cardiogenic shock severity. J Crit Care. 2022;68:50-8. doi: 10.1016/j.jcrc.2021.12.005.
Lukić I, Mihić D, Varžić SC, Relatić KS, Zibar L, Loinjak D, et al. Septic Cardiomyopathy. Rev Cardiovasc Med. 2024;25(1):23. doi: 10.31083/j. rcm2501023.
van Diepen S, Pöss J, Senaratne JM, Gage A, Morrow DA. Mixed Cardiogenic Shock: A Proposal for Standardized Classification, a Hemodynamic Definition, and Framework for Management. Circulation. 2024;150(18):1459-68. doi: 10.1161/CIRCULATIONAHA.124.069508.
Menon V, Slater JN, White HD, Sleeper LA, Cocke T, Hochman JS. Acute myocardial infarction complicated by systemic hypoperfusion without hypotension: report of the SHOCK trial registry. Am J Med. 2000;108(5):374-80. doi: 10.1016/s0002-9343(00)00310-7.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 The journal is headline of the first publication, then the author giving credit to the first publication.

This work is licensed under a Creative Commons Attribution 4.0 International License.