Original Article
Arterial
lactate levels and their prognostic value in patients undergoing pulmonary
thromboendarterectomy
Niveles
de lactato arterial y su valor pronóstico en pacientes sometidos a tromboendarterectomía
pulmonar
![]() Cristhian
Felipe Ramírez-Ramos 1,a,*
Cristhian
Felipe Ramírez-Ramos 1,a,*
https://orcid.org/0000-0002-3617-4585
Clara Inés Saldarriaga-Giraldo ![]() 2,b
2,b
https://orcid.org/0000-0002-5945-1127
Manuela Yepes-Calderón3,c
Gustavo Adolfo Castilla–Agudelo1,d
https://orcid.org/0000-0002-0957-2318
Mateo Aránzazu Uribe ![]() 4,d
4,d
https://orcid.org/0000-0002-3296-7414
Santiago Saldarriaga Betancur ![]() 4,d
4,d
https://orcid.org/0000-0001-8232-8939
Paulina Casto5,e, Catalina Gallego2,b
Alejandro Londoño6,f
Juan Camilo Rendon-Isaza7,g
Eliana Cañas8,h
Álvaro Porras9,i
Juan David Uribe-Molano9
DOI: https://doi.org/10.47487/apcyccv.v2i2.131
Abstract
Objective. Evaluate the change of
lactate levels and its prognostic role in the postoperative period of patients
undergoing pulmonary thromboendarterectomy. Methods. Retrospective study
between 2001 and 2019. Patients older
than 18 years and who underwent pulmonary thromboendarterectomy were included.
The U Mann Whitney test was performed to evaluate the change between lactate levels,
and Cox regression analysis to evaluate the relationship with mortality. Areas
under the curve were constructed for lactate levels. Results. Seventy-three
patients were operated on during the study period. Median age was 51 years, 55%
female. The median lactate on days 1 was 4.65 mml/L and on day 2 it was 1.62
mml/L with a change of 2.87 mml/L. No differences were found between the levels
measured on day 1 and 2 between the people who died and those who did not on
day 30. In the multivariate regression of COX, no relationship with mortality
was found. The area under the curve shows regular performance on both day 1 and
day 2 in predicting mortality outcomes. Conclusions. The behavior of the
lactate in patients undergoing pulmonary thromboendarterectomy shows a rapid
change during the first hours after the procedure. No role was found as a
predictor of mortality neither in-hospital nor in follow-up.
Keywords. Pulmonary
Hypertension; Pulmonary Embolism; Endarterectomy; Lactic Acid (source: MeSH
NLM).
Resumen
Objetivo. Evaluar el cambio de los
niveles de lactato y su rol pronóstico en el posoperatorio de pacientes
sometidos a tromboendarterectomía pulmonar. Métodos. Estudio retrospectivo
entre 2001 y 2019. Se incluyeron pacientes mayores de 18 años que fueron
sometidos a tromboendarterectomía pulmonar. Para evaluar el cambio entre los
niveles de lactato se realizó la prueba de U Mann Whitney. Para evaluar la
relación con la mortalidad se realizó un análisis multivariado de Cox. Se
construyeron áreas bajo la curva para los niveles de lactato. Resultados.
Setenta y tres pacientes fueron operados durante el período de estudio. La
mediana de edad fue de 51 años, 55% mujeres. La mediana de lactato en el día 1
fue de 4,65 mmL/L y en el día 2 fue de 1,62 mmL/L con un cambio de 2,87 mmL/L.
No se encontraron diferencias entre los niveles medidos el día 1 y 2 entre las
personas que murieron y las que no al día 30 hospitalario. En la regresión
multivariada de COX no se encontró relación con la mortalidad. El área bajo la
curva muestra un desempeño regular tanto
en el día 1 como en el día 2 para predecir el resultado de la mortalidad en
especial intrahospitalaria. Conclusiones. El comportamiento del lactato en
pacientes sometidos a tromboendarterectomía pulmonar muestra un cambio rápido
durante las primeras horas posteriores al procedimiento. No se encontró que sea
un predictor de mortalidad ni hospitalaria ni durante el seguimiento.
Palabras
clave.
Hipertensión Pulmonar; Embolia Pulmonar; Endarterectomía; Ácido Láctico
(fuente: DeCS BIREME).
Although the exact incidence and prevalence is unknown, it is estimated that
around 4-5% of patients who suffer an acute pulmonary embolism develop chronic thromboembolic
pulmonary hypertension (CTPH). This disease is characterized by intraluminal
organization of the thrombus, fibrotic scar-like stenosis, and vascular
remodeling (1). This disease is associated with a poor prognosis and when the
mean pulmonary pressure reaches 50 mmHg or more, 3-year mortality is 90% (2).
Pulmonary thromboendarterectomy
remains the preferred treatment and is a potentially curative option for
patients with chronic thromboembolic pulmonary hypertension. Despite this, only
0.9 to 1 procedure are performed per million inhabitants in the United States
and 1.7 per million in European countries (3). The benefit of the
procedure has been established in multiple series, achieving improvement in
functional status, exercise capacity, and hemodynamic variables with mortality rates of the procedure in
high-experience centers of 2.2% (4).
Cardiopulmonary bypass (CPB) using a
heart-lung machine (HLM) represents a standard technique in modern cardiac
surgery. CPB provides adequate systemic oxygenation and perfusion during
cardiac operation through the adjustment of flow rate, temperature, oxygen
concentration, and hemoglobin level (5). Intraoperative events, including
surgical techniques, methods used in myocardial protection, and CPB, can affect
surgical outcomes. Altered mental status and decreased urine output are signs
of tissue hypoperfusion; however, an adequate and timely assessment of such
signs cannot be carried out during cardiac operation. Lactate is an end product
of anaerobic glycolysis from oxygen deficit and tissue hypoperfusion. It
is an obtainable surrogate marker of
tissue hypoxia and disease severity and is considered an index marker of
circulatory shock (6).
Since the early studies by Weil (7)
and other authors (8), lactate concentrations have been used extensively as a
marker in critically ill patients (9). Even elevations of > 1.5 mmol/L have
been associated with higher mortality rates (10). In the particular shock
scenario, regardless of its mechanism, this molecule is a marker of the hypoperfusion state and
the degree of increase is directly related to the severity and higher mortality
rates (11).
Moreover, an elevated lactate level is
observed during cardiac operation with CPB in a bimodal distribution. Type A
hyperlactatemia can occur during or soon after the initiation of CPB tissue due
to hypoperfusion. Meanwhile, type B hyperlactatemia can be observed 4–14 h
after surgery when a patient is admitted to an intensive care unit (ICU) under
adequate oxygen delivery owing to increased substrate utilization (12). A
higher lactate level during CPB reflects inadequate tissue perfusion, which may
be associated with poor surgical outcomes Increased lactate concentrations are also associated with an increased risk of morbidity
and death in pediatric patients undergoing
cardiac surgery (13) as well as in patients undergoing coronary bypass procedures (CABG) (14). Hyperlactatemia (defined as levels> 2
mmol/L) has been reported in 36% of cardiac
surgery patients and is a predictor of death (15).
Data on the kinetics of this molecule
and its prognostic significance are unknown in patients undergoing pulmonary
thromboendarterectomy. The objective
of the present study was to evaluate the change of
lactate and establish its prognostic role as a predictor of global and
in-hospital death in patients undergoing pulmonary thromboendarterectomy in a
cardiovascular referral center.
Materials and methods
Retrospective cohort
study between January
2001 and November 2019 of patients > 18 years of age undergoing
pulmonary thromboendarterectomy in a referral center for cardiovascular care.
The patients were chosen for the procedure according to a multidisciplinary
evaluation with the intervention of
cardiovascular surgeons, cardiologists, specialists in heart failure and
pulmonologists from the pulmonary hypertension clinic, considering functional
class, accessibility of thrombotic lesions, hemodynamic status and
comorbidities. Data were collected from the index hospitalization, related to
the surgical procedure and its complications, including mortality. Lactate levels were recorded immediately
after the surgical procedure and 24
hours later. The data included in the analysis were demographic and clinical
variables, as well as characteristics related to the procedure and change in
lactate levels. Continuous variables are presented as mean
with standard deviation
(SD) or as median and interquartile range [IQR] according to their
distribution.
To evaluate the change (delta)
between lactate levels
on day 1 and day 2, the U Mann Whitney test was performed. To evaluate
whether the change between day 1 and day 2 in lactate levels was associated
with global mortality as
in-hospital (first 30 days), a
Cox regression analysis was performed. The model included age, sex, functional
class, hemodynamic data such as pre and postsurgical mean pulmonary
arterial pressure, pre- and postsurgical pulmonary and systemic
vascular resistances, surgical times, mechanical ventilation time, the presence
of edema of reperfusion and length of stay in intensive care unit. The Hazard
Ratio (HR) calculated for lactate levels were adjusted for the variables
included in the model. Areas under the curve (AUC) were constructed to assess
lactate performance as
a predictor of mortality.
In addition, a
linear regression was
performed to establish whether lactate levels were related to days of mechanical
ventilation. All analyzes were carried out using the SPSS version 22.0
statistical program.
The present study was approved by the
institutional ethics committee and the Universidad Pontificia Bolivariana
(minute 16 2020) and Clínica CardioVID, according to the research operative
manual and resolution 8430/1993.
Results
(Central figure)
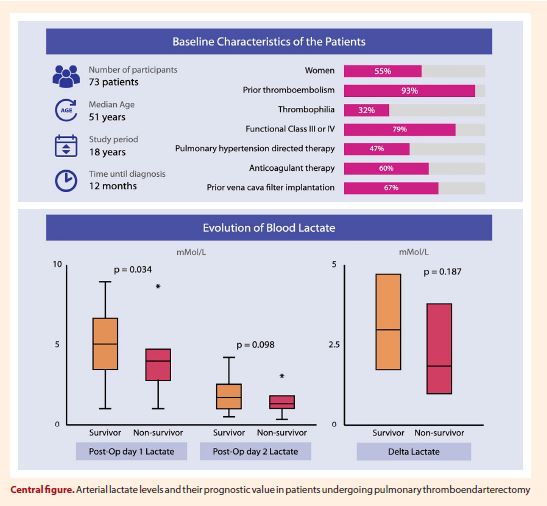
Over a period of 18 years, 73 patients
underwent pulmonary thromboendarterectomy. The median age was 51 years, 55% of
the patients were women; 93% of the population had a history of pulmonary
thromboembolism and 32% history of
thrombophilia, the most common was antiphospholipid syndrome (23%). The most
frequent presenting symptoms were dyspnea and fatigue; 20% presented syncopal
episodes, with a time between the onset of symptoms and their diagnosis of 12
months. Most of the patients had marked symptoms, 79% being in functional class
III and IV. The median pressure of the pulmonary artery was 50 mmHg in the
right catheterization, with pulmonary vascular resistance of 640
dyn.sec.cm-5 and systemic
resistance of 1600 dyn.sec.cm-5. A 46.5% of the
population received specific
treatment for pulmonary hypertension, sildenafil (n: 25; 34.2%) and bosentan (n:
11; 15%) being the most frequently used (14 in combination therapy and of these
6 received the sildenafil-bosentan combination). A little more than half were
in anticoagulation management (60%), half were taking warfarin and the remaining were on direct
anticoagulants (rivaroxaban and apixaban
the most frequent). Prior to the procedure, two- thirds of the population
received an inferior vena cava filter implant.
Regarding the surgical procedure, the
median perfusion time was 292 minutes, the aortic clamp time was 120 minutes,
and the circulatory arrest time was 64 minutes. Additional procedures were
performed in 17 patients (23%), with tricuspid plasty and the correction of an
atrial septal defect being the most frequent; only 2 patients required
coronary artery bypass graft
surgery. Regarding the
hemodynamic parameters after the surgical intervention, there was a
significant decrease in parameters such as pulmonary artery systolic pressure
(median 47 mmHg; change of 46%), mean pulmonary artery pressure (median 30
mmHg; change of 40%), pulmonary artery diastolic pressure (median 18 mmHg;
43.8% change), systemic vascular resistance (SVR) (median 916 dyn.sec.cm-5;
42.8% change) and pulmonary vascular resistance (PVR) (median 136 dyn.sec.cm-5;
79% change).
Complications related to the procedure occurred in a
minority of cases (10%), of which vascular lesions were the main ones; no patient
died during the procedure. Half of the patients required
inotropic support (n: 39; 53%) after
the procedure and in
a lesser percentage vasopressor support (n: 32; 43%). 43% of the patients
had reperfusion edema. The median stay in the intensive care unit was 6 days [IQR: 3-13], with a
median of 2 days of mechanical ventilation [IQR:1-6] and a total time of hospitalization of 20 days [IQR:14-29].
Regarding mortality, there were 14
events (19.17%) in the study
period. Most of these (n: 9; 12.32%) occurred at 30 days, septic shock being
the main cause followed by cardiogenic etiology. Five deaths were recorded
during the first 6 months; of these 3 due to pulmonary infectious complications
and in 2 cases the cause could not be established.
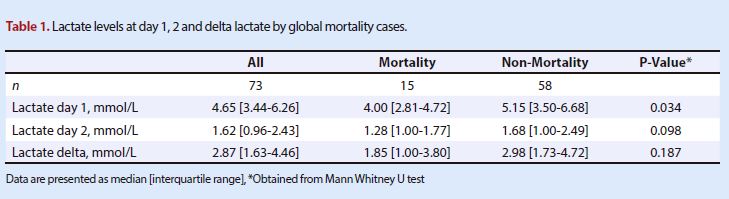
The median lactate on day 1 was 4.65
mmol/L and on day 2 it was 1.62 mmol/L
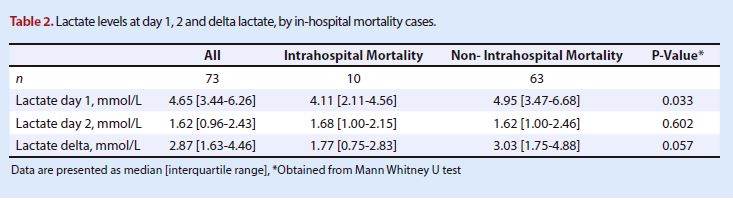
with a change of 2.87 mmol/L, changes that were not significant. When
performing the analysis between patients who
died in-hospital (first
30 days) and
those who did not obtain values
for the first day of 4.11 mmol/L and 4.95 mmol/L respectively. The value at day
2 was
1.68 mmol/L for the patients who died and 1.62 for those
who did not die, with a delta of 1.77 mmol/L for the first group
and 3.03 mmol/L for the second (Table
1). The variations in lactate levels stratified by results (mortality,
in-hospital mortality) did not show statistically significant changes (Table
2).
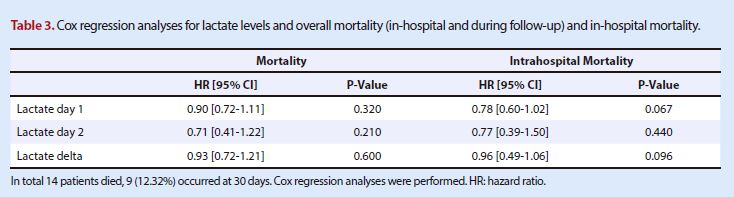
In the multivariate Cox regression, no
relationship was found with global or in-hospital mortality between the levels
on day 1, or on day 2, such as the absolute change (Table 3). Lactate levels
did not show a relationship with the time of invasive mechanical ventilation,
with Standardized β values of -0.27 (95% CI -1.81 to -0.16, p=0.020) for
the day 1; -0.25 (95% CI -3.87 to -0.14, p=0.040) for the day 2 and -0.18 (95%
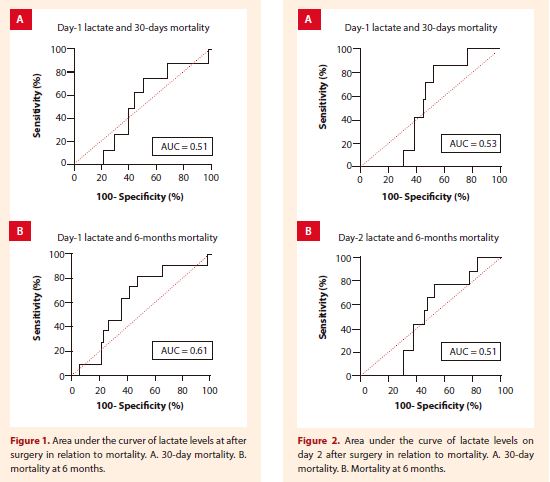
CI -0.16 to 0.21, p=0.130) for the lactate delta. The area under the curve were
0.51 for 30-days mortality and 0.61 for 6-months mortality in day 1 (Figure 1),
and 0.53 for 30-days mortality and 0.51 for 6-months mortality in day 2 (Figure
2) to predict the mortality outcomes.
Discussion
The results of the behavior and kinetics
of lactate are presented as its prognostic performance
in a population undergoing pulmonary thromboendarterectomy in a referral
center. The analysis between lactate level and mechanical ventilation did not
show a relationship, mentioning the fact
that the average number of days of mechanical ventilation was 2 days, with a
significant percentage of
reperfusion edema. The lactate
performance assessed by the area under the curve is generally regular both on
day 1 and on day 2 in relation to the outcome of death. It is necessary to
confirm these results in prospective studies with an adequate follow-up time
and a larger sample size.
In a cardiac surgery, extracorporeal
circulation (EC) allows surgeons to treat a wide range of heart disease while
machines maintain circulation and oxygenation of human blood (5). Initially,
the creation of embolic
particles in response to trauma
was a common adverse effect of
EC (16). However, with
the passage of time, biomaterials were created, and pharmacological therapies
were implemented that reduced these potential adverse events,
which in turn improved
the results of the therapy. Despite
contemporary success,
patients undergoing cardiac surgery
have
complications related to the inappropriate inflammatory response developed.
Potential triggers related to this response have been endotoxemia,
ischemia-reperfusion injury, and exposure of the blood to non-endothelial
surfaces (17). There is an increase in the recruitment of leukocytes and
proinflammatory cytokines, secondary to the activation of the cellular and
humoral immune systems (18). The complications associated with the development
of this systemic inflammatory response syndrome are: myocardial dysfunction,
acute renal failure, neurological dysfunction, respiratory failure, bleeding and
finally multiple organ failure (MOF)
(18), that has been correlated with an increase in the probability of dying as
well as in morbidity in patients undergoing cardiovascular surgery (18).
Hyperlactatemia (HL) in patients who undergo
cardiac surgery with CPB can be due to tissue hypoxia, nonhypoxic causes such
as drug therapy, cardioplegia solution, hypothermia, and CPB itself (19).
Demers et al.(20), found that in adult patients undergoing cardiac surgery, HL
is detected in 10–20% of patients and was associated with significant
postoperative morbidity and mortality.
In a study done by Broder and Weil, more than 88% of patients who had blood a
lactate level of > 4.0 mmol/L had a high risk of mortality due to
circulatory shock (7). The same authors documented that the chances of survival
from shock declines from 90 to 10% as blood lactate levels escalates from 2.0
to 8.0 mmol/L (8).
Patients undergoing cardiac surgery
under CPB, despite having normal arterial blood gases (ABGs), may still
experience lactic acidosis secondary to tissue hypoperfusion. Therefore, monitoring
blood lactate levels in cardiac surgery patients might be more sensitive than
ABG analysis alone and will thereby help in early detection of an imbalance
between oxygen supply and demand. The SIRS associated with
CPB and its previously mentioned complications may be an additional cause of
tissue hypoperfusion and hyperlactatemia.
To date there are no data on the
behavior of the lactate in patients undergoing pulmonary thromboendarterectomy.
The findings of the population show
that, despite the
requirement of a significant proportion of vasoactive supports, the
patients achieved concentrations lower than 2 mmol/L during day 2 after the
intervention. Notably, patients in the in-hospital mortality group presented
lower levels on day 1 compared to those who
did not die, which is consistent with a lower delta between day 1 and 2 in this group (1.77 mmol/L)
compared to patients that survived (3.03 mmol/L). However, no association with
mortality could be established, even when adjusted to clinical, surgical and
hemodynamic variables of interest.
The present study has the following
limitations: the retrospective nature of the study means that all biases or confounding
factors cannot be controlled for; the
small number of patients and
events makes the findings regarding mortality and complications not
generalizable and does not rule out an existing relationship.The sample size
could be a limitation for having a study with adequate power. The levels were
only measured at two points during the first day and 24 hours after it, so the
lack of relationship with the outcomes can be explained by the compound’s ownkinetics
and the lack of data in days after or close to the events. Also, a relationship
was not made with the blood pH level as with other metabolic parameters in the
studied population.
Conclusions
Lactate behavior in patients
undergoing pulmonary thromboendarterectomy for chronic thromboembolic pulmonary
disease shows a rapid change during the first hours after the surgical
procedure and no relationship with in-hospital mortality was found in the
present study. However, studies with a larger population and more frequent
measurements should be carried out to validate
these results.
Authors’ Contributions: CFRR, CISG,
JCRI, contributed to the acquisition of data, to the conception or design of
the study and drafted the manuscript.
GACA, MAU, SSB, PC, CG, AL, AP, JDUM,
MYC: contributed interpretation of data and critical revision of the article
for important intellectual content.
Acknowledgement: Dr. Carlos Pereda for
the central image.
Referencias
bibliográficas
1. Madani MM.
Surgical Treatment of Chronic Thromboembolic Pulmonary Hypertension: Pulmonary
Thromboendarterectomy. Methodist Debakey Cardiovasc J. 2016;12(4):213-218. doi:
10.14797/ mdcj-12-4-213.
2. Riedel M,
Stanek V, Widimsky J, Prerovsky I. Longterm follow-up of patients with pulmonary thromboembolism.
Late prognosis and evolution of hemodynamic and respiratory data. Chest.
1982;81(2):151-8. doi: 10.1378/chest.81.2.151.